Learning Objectives
By the end of this section, you will be able to:
- Describe the nature and symptoms of attention deficit/hyperactivity disorder and autism spectrum disorder
- Discuss the prevalence and factors that contribute to the development of these disorders
Most of the disorders we have discussed so far are typically diagnosed in adulthood, although they can and sometimes do occur during childhood. However, there are a group of conditions that, when present, are diagnosed early in childhood, often before the time a child enters school. These conditions are listed in the DSM-5 as neurodevelopmental disorders, and they involve developmental problems in personal, social, academic, and intellectual functioning (APA, 2013). In this section, we will discuss two such disorders: attention deficit/ hyperactivity disorder and autism.
ATTENTION DEFICIT/HYPERACTIVITY DISORDER
Diego is always active, from the time he wakes up in the morning until the time he goes to bed at night. His mother reports that he came out the womb kicking and screaming, and he has not stopped moving since. He has a sweet disposition, but always seems to be in trouble with his teachers, parents, and after-school program counselors. He seems to accidently break things; he lost his jacket three times last winter, and he never seems to sit still. His teachers believe he is a smart child, but he never finishes anything he starts and is so impulsive that he does not seem to learn much in school.
Diego likely has attention deficit/hyperactivity disorder (ADHD). The symptoms of this disorder were first described by Hans Hoffman in the 1920s. While taking care of his son while his wife was in the hospital giving birth to a second child, Hoffman noticed that the boy had trouble concentrating on his homework, had a short attention span, and had to repeatedly go over easy homework to learn the material (Jellinek Herzog, 1999). Later, it was discovered that many hyperactive children—those who are fidgety, restless, socially disruptive, and have trouble with impulse control—also display short attention spans, problems with concentration, and distractibility. By the 1970s, it had become clear that many children who display attention problems often also exhibit signs of hyperactivity. In recognition of such findings, the DSM-III (published in 1980) included a new disorder: attention deficit disorder with and without hyperactivity, now known as attention deficit/hyperactivity disorder (ADHD).
A child with ADHD shows a constant pattern of inattention and/or hyperactive and impulsive behavior that interferes with normal functioning (APA, 2013). Some of the signs of inattention include great difficulty with and avoidance of tasks that require sustained attention (such as conversations or reading), failure to follow instructions (often resulting in failure to complete school work and other duties), disorganization (difficulty keeping things in order, poor time management, sloppy and messy work), lack of attention to detail, becoming easily distracted, and forgetfulness. Hyperactivity is characterized by excessive movement, and includes fidgeting or squirming, leaving one’s seat in situations when remaining seated is expected, having trouble sitting still (e.g., in a restaurant), running about and climbing on things, blurting out responses before another person’s question or statement has been completed, difficulty waiting one’s turn for something, and interrupting and intruding on others. Frequently, the hyperactive child comes across as noisy and boisterous. The child’s behavior is hasty, impulsive, and seems to occur without much forethought; these characteristics may explain why adolescents and young adults diagnosed with ADHD receive more traffic tickets and have more automobile accidents than do others (Thompson, Molina, Pelham, Gnagy, 2007).
ADHD occurs in about 5% of children (APA, 2013). On the average, boys are 3 times more likely to have ADHD than are girls; however, such findings might reflect the greater propensity of boys to engage in aggressive and antisocial behavior and thus incur a greater likelihood of being referred to psychological clinics (Barkley, 2006). Children with ADHD face severe academic and social challenges. Compared to their non-ADHD counterparts, children with ADHD have lower grades and standardized test scores and higher rates of expulsion, grade retention, and dropping out (Loe Feldman, 2007). they also are less well- liked and more often rejected by their peers (Hoza et al., 2005).
Previously, ADHD was thought to fade away by adolescence. However, longitudinal studies have suggested that ADHD is a chronic problem, one that can persist into adolescence and adulthood (Barkley, Fischer, Smallish, Fletcher, 2002). A recent study found that 29.3% of adults who had been diagnosed with ADHD decades earlier still showed symptoms (Barbaresi et al., 2013). Somewhat troubling, this study also reported that nearly 81% of those whose ADHD persisted into adulthood had experienced at least one other comorbid disorder, compared to 47% of those whose ADHD did not persist.
Life Problems from ADHD
Children diagnosed with ADHD face considerably worse long-term outcomes than do those children who do not receive such a diagnosis. In one investigation, 135 adults who had been identified as having ADHD symptoms in the 1970s were contacted decades later and interviewed (Klein et al., 2012). Compared to a control sample of 136 participants who had never been diagnosed with ADHD, those who were diagnosed as children:
- had worse educational attainment (more likely to have dropped out of high school and less likely to have earned a bachelor’s degree);
- had lower socioeconomic status;
- held less prestigious occupational positions;
- were more likely to be unemployed;
- made considerably less in salary;
- scored worse on a measure of occupational functioning (indicating, for example, lower job satisfaction, poorer work relationships, and more firings);
- scored worse on a measure of social functioning (indicating, for example, fewer friendships and less involvement in social activities);
- were more likely to be divorced; and
- were more likely to have non-alcohol-related substance abuse problems. (Klein et al., 2012) Longitudinal studies also show that children diagnosed with ADHD are at higher risk for substance abuse
problems. One study reported that childhood ADHD predicted later drinking problems, daily smoking, and use of marijuana and other illicit drugs (Molina Pelham, 2003). The risk of substance abuse problems appears to be even greater for those with ADHD who also exhibit antisocial tendencies (Marshal Molina, 2006).
Causes of ADHD
Family and twin studies indicate that genetics play a significant role in the development of ADHD. Burt (2009), in a review of 26 studies, reported that the median rate of concordance for identical twins was .66 (one study reported a rate of .90), whereas the median concordance rate for fraternal twins was .20. This study also found that the median concordance rate for unrelated (adoptive) siblings was .09; although this number is small, it is greater than 0, thus suggesting that the environment may have at least some influence. Another review of studies concluded that the heritability of inattention and hyperactivity were 71% and 73%, respectively (Nikolas Burt, 2010).
The specific genes involved in ADHD are thought to include at least two that are important in the regulation of the neurotransmitter dopamine (Gizer, Ficks, Waldman, 2009), suggesting that dopamine may be important in ADHD. Indeed, medications used in the treatment of ADHD, such as methylphenidate (Ritalin) and amphetamine with dextroamphetamine (Adderall), have stimulant qualities and elevate dopamine activity. People with ADHD show less dopamine activity in key regions of the brain, especially those associated with motivation and reward (Volkow et al., 2009), which provides support to the theory that dopamine deficits may be a vital factor in the development this disorder (Swanson et al., 2007).
Brain imaging studies have shown that children with ADHD exhibit abnormalities in their frontal lobes, an area in which dopamine is in abundance. Compared to children without ADHD, those with ADHD appear to have smaller frontal lobe volume, and they show less frontal lobe activation when performing mental tasks. Recall that one of the functions of the frontal lobes is to inhibit our behavior. Thus, abnormalities in this region may go a long way toward explaining the hyperactive, uncontrolled behavior of ADHD.
By the 1970s, many had become aware of the connection between nutritional factors and childhood behavior. At the time, much of the public believed that hyperactivity was caused by sugar and food additives, such as artificial coloring and flavoring. Undoubtedly, part of the appeal of this hypothesis was that it provided a simple explanation of (and treatment for) behavioral problems in children. A statistical review of 16 studies, however, concluded that sugar consumption has no effect at all on the behavioral and cognitive performance of children (Wolraich, Wilson, White, 1995). Additionally, although food additives have been shown to increase hyperactivity in non-ADHD children, the effect is rather small (McCann et al., 2007). Numerous studies, however, have shown a significant relationship between exposure to nicotine in cigarette smoke during the prenatal period and ADHD (Linnet et al., 2003). Maternal smoking during pregnancy is associated with the development of more severe symptoms of the disorder (Thakur et al., 2013).
Is ADHD caused by poor parenting? Not likely. Remember, the genetics studies discussed above suggested that the family environment does not seem to play much of a role in the development of this disorder; if it did, we would expect the concordance rates to be higher for fraternal twins and adoptive siblings than has been demonstrated. All things considered, the evidence seems to point to the conclusion that ADHD is triggered more by genetic and neurological factors and less by social or environmental ones.
AUTISM SPECTRUM DISORDER
A seminal paper published in 1943 by psychiatrist Leo Kanner described an unusual neurodevelopmental condition he observed in a group of children. He called this condition early infantile autism, and it was characterized mainly by an inability to form close emotional ties with others, speech and language abnormalities, repetitive behaviors, and an intolerance of minor changes in the environment and in normal routines (Bregman, 2005). What the DSM-5 refers to as autism spectrum disorder today, is a direct extension of Kanner’s work.
Autism spectrum disorder is probably the most misunderstood and puzzling of the neurodevelopmental disorders. Children with this disorder show signs of significant disturbances in three main areas: (a) deficits in social interaction, (b) deficits in communication, and (c) repetitive patterns of behavior or interests. These disturbances appear early in life and cause serious impairments in functioning (APA, 2013). The child with autism spectrum disorder might exhibit deficits in social interaction by not initiating conversations with other children or turning their head away when spoken to. These children do not make eye contact with others and seem to prefer playing alone rather than with others. In a certain sense, it is almost as though these individuals live in a personal and isolated social world others are simply not privy to or able to penetrate. Communication deficits can range from a complete lack of speech, to one word responses (e.g., saying “Yes” or “No” when replying to questions or statements that require additional elaboration), to echoed speech (e.g., parroting what another person says, either immediately or several hours or even days later), to difficulty maintaining a conversation because of an inability to reciprocate others’ comments. These deficits can also include problems in using and understanding nonverbal cues (e.g., facial expressions, gestures, and postures) that facilitate normal communication.
Repetitive patterns of behavior or interests can be exhibited a number of ways. The child might engage in stereotyped, repetitive movements (rocking, head-banging, or repeatedly dropping an object and then picking it up), or she might show great distress at small changes in routine or the environment. For example, the child might throw a temper tantrum if an object is not in its proper place or if a regularly- scheduled activity is rescheduled. In some cases, the person with autism spectrum disorder might show highly restricted and fixated interests that appear to be abnormal in their intensity. For instance, the person might learn and memorize every detail about something even though doing so serves no apparent purpose. Importantly, autism spectrum disorder is not the same thing as intellectual disability, although these two conditions are often comorbid. The DSM-5 specifies that the symptoms of autism spectrum disorder are not caused or explained by intellectual disability.
Life Problems From Autism Spectrum Disorder
Autism spectrum disorder is referred to in everyday language as autism; in fact, the disorder was termed “autistic disorder” in earlier editions of the DSM, and its diagnostic criteria were much narrower than those of autism spectrum disorder. The qualifier “spectrum” in autism spectrum disorder is used to indicate that individuals with the disorder can show a range, or spectrum, of symptoms that vary in their magnitude and severity: some severe, others less severe. The previous edition of the DSM included a diagnosis of Asperger’s disorder, generally recognized as a less severe form of autistic disorder; individuals diagnosed with Asperger’s disorder were described as having average or high intelligence and a strong vocabulary, but exhibiting impairments in social interaction and social communication, such as talking only about their special interests (Wing, Gould, Gillberg, 2011). However, because research has failed to demonstrate that Asperger’s disorder differs qualitatively from autistic disorder, the DSM-5 does not include it, which is prompting concerns among some parents that their children may no longer be eligible for special services (“Asperger’s Syndrome Dropped,” 2012). Some individuals with autism spectrum disorder, particularly those with better language and intellectual skills, can live and work independently as adults. However, most do not because the symptoms remain sufficient to cause serious impairment in many realms of life (APA, 2013).
Link to Learning
Here is an instructive and poignant video highlighting severe autism.
Currently, estimates indicate that nearly 1 in 88 children in the United States has autism spectrum disorder; the disorder is 5 times more common in boys (1 out of 54) than girls (1 out of 252) (CDC, 2012). Rates of autistic spectrum disorder have increased dramatically since the 1980s. For example, California saw an increase of 273% in reported cases from 1987 through 1998 (Byrd, 2002); between 2000 and 2008, the rate of autism diagnoses in the United States increased 78% (CDC, 2012). Although it is difficult to interpret this increase, it is possible that the rise in prevalence is the result of the broadening of the diagnosis, increased efforts to identify cases in the community, and greater awareness and acceptance of the diagnosis. In addition, mental health professionals are now more knowledgeable about autism spectrum disorder and are better equipped to make the diagnosis, even in subtle cases (Novella, 2008).
Dig Deeper
Why Is the Prevalence Rate of ADHD Increasing?
Many people believe that the rates of ADHD have increased in recent years, and there is evidence to support this contention. In a recent study, investigators found that the parent-reported prevalence of ADHD among children (4–17 years old) in the United States increased by 22% during a 4-year period, from 7.8% in 2003 to 9.5% in 2007 (CDC, 2010). Over time this increase in parent-reported ADHD was observed in all sociodemographic groups and was reflected by substantial increases in 12 states (Indiana, North Carolina, and Colorado were the top three). The increases were greatest for older teens (ages 15–17), multiracial and Hispanic children, and children with a primary language other than English. Another investigation found that from 1998–2000 through 2007–2009 the parent-reported prevalence of ADHD increased among U.S. children between the ages of 5–17 years old, from 6.9% to 9.0% (Akinbami, Liu, Pastor, & Reuben, 2011).
A major weakness of both studies was that children were not actually given a formal diagnosis. Instead, parents were simply asked whether or not a doctor or other health-care provider had ever told them their child had ADHD; the reported prevalence rates thus may have been affected by the accuracy of parental memory. Nevertheless, the findings from these studies raise important questions concerning what appears to be a demonstrable rise in the prevalence of ADHD. Although the reasons underlying this apparent increase in the rates of ADHD over time are poorly understood and, at best, speculative, several explanations are viable:
- ADHD may be over-diagnosed by doctors who are too quick to medicate children as a behavior treatment.
- There is greater awareness of ADHD now than in the past. Nearly everyone has heard of ADHD, and most parents and teachers are aware of its key symptoms. Thus, parents may be quick to take their children to a doctor if they believe their child possesses these symptoms, or teachers may be more likely now than in the past to notice the symptoms and refer the child for evaluation.
- The use of computers, video games, iPhones, and other electronic devices has become pervasive among children in the early 21st century, and these devices could potentially shorten children’s attentions spans. Thus, what might seem like inattention to some parents and teachers could simply reflect exposure to too much technology.
- ADHD diagnostic criteria have changed over time.
Causes of Autism Spectrum Disorder
Early theories of autism placed the blame squarely on the shoulders of the child’s parents, particularly the mother. Bruno Bettelheim (an Austrian-born American child psychologist who was heavily influenced by Sigmund Freud’s ideas) suggested that a mother’s ambivalent attitudes and her frozen and rigid emotions toward her child were the main causal factors in childhood autism. In what must certainly stand as one of the more controversial assertions in psychology over the last 50 years, he wrote, “I state my belief that the precipitating factor in infantile autism is the parent’s wish that his child should not exist” (Bettelheim, 1967, p. 125). As you might imagine, Bettelheim did not endear himself to a lot of people with this position; incidentally, no scientific evidence exists supporting his claims.
The exact causes of autism spectrum disorder remain unknown despite massive research efforts over the last two decades (Meek, Lemery-Chalfant, Jahromi, Valiente, 2013). Autism appears to be strongly influenced by genetics, as identical twins show concordance rates of 60%–90%, whereas concordance rates for fraternal twins and siblings are 5%–10% (Autism Genome Project Consortium, 2007). Many different genes and gene mutations have been implicated in autism (Meek et al., 2013). Among the genes involved are those important in the formation of synaptic circuits that facilitate communication between different areas of the brain (Gauthier et al., 2011). A number of environmental factors are also thought to be associated with increased risk for autism spectrum disorder, at least in part, because they contribute to new mutations. These factors include exposure to pollutants, such as plant emissions and mercury, urban versus rural residence, and vitamin D deficiency (Kinney, Barch, Chayka, Napoleon, Munir, 2009).
Child Vaccinations and Autism Spectrum Disorder
In the late 1990s, a prestigious medical journal published an article purportedly showing that autism is triggered by the MMR (measles, mumps, and rubella) vaccine. These findings were very controversial and drew a great deal of attention, sparking an international forum on whether children should be vaccinated. In a shocking turn of events, some years later the article was retracted by the journal that had published it after accusations of fraud on the part of the lead researcher. Despite the retraction, the reporting in popular media led to concerns about a possible link between vaccines and autism persisting. A recent survey of parents, for example, found that roughly a third of respondents expressed such a concern (Kennedy, LaVail, Nowak, Basket, Landry, 2011); and perhaps fearing that their children would develop autism, more than 10% of parents of young children refuse or delay vaccinations (Dempsey et al., 2011). Some parents of children with autism mounted a campaign against scientists who refuted the vaccine-autism link. Even politicians and several well-known celebrities weighed in; for example, actress Jenny McCarthy (who believed that a vaccination caused her son’s autism) co-authored a book on the matter. However, there is no scientific evidence that a link exists between autism and vaccinations (Hughes, 2007). Indeed, a recent study compared the vaccination histories of 256 children with autism spectrum disorder with that of 752 control children across three time periods during their first two years of life (birth to 3 months, birth to 7 months, and birth to 2 years) (DeStefano, Price, Weintraub, 2013). At the time of the study, the children were between 6 and 13 years old, and their prior vaccination records were obtained. Because vaccines contain immunogens (substances that fight infections), the investigators examined medical records to see how many immunogens children received to determine if those children who received more immunogens were at greater risk for developing autism spectrum disorder. The results of this study, a portion of which are shown in Figure 3.20, clearly demonstrate that the quantity of immunogens from vaccines received during the first two years of life were not at all related to the development of autism spectrum disorder. There is not a relationship between vaccinations and autism spectrum disorders.
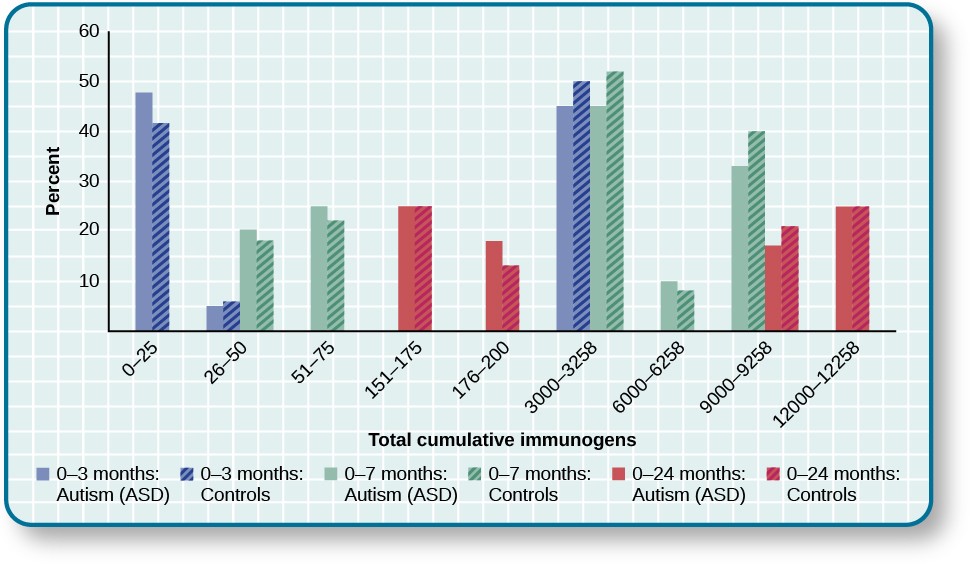
Figure 3.20 In terms of their exposure to immunogens in vaccines, overall, there is not a significant difference between children with autism spectrum disorder and their age-matched controls without the disorder (DeStefano et al., 2013).
Why does concern over vaccines and autism spectrum disorder persist? Since the proliferation of the Internet in the 1990s, parents have been constantly bombarded with online information that can become magnified and take on a life of its own. The enormous volume of electronic information pertaining to autism spectrum disorder, combined with how difficult it can be to grasp complex scientific concepts, can make separating good research from bad challenging (Downs, 2008). Notably, the study that fueled the controversy reported that 8 out of 12 children—according to their parents—developed symptoms consistent with autism spectrum disorder shortly after receiving a vaccination. To conclude that vaccines cause autism spectrum disorder on this basis, as many did, is clearly incorrect for a number of reasons, not the least of which is because correlation does not imply causation, as you’ve learned.
Additionally, as was the case with diet and ADHD in the 1970s, the notion that autism spectrum disorder is caused by vaccinations is appealing to some because it provides a simple explanation for this condition. Like all disorders, however, there are no simple explanations for autism spectrum disorder. Although the research discussed above has shed some light on its causes, science is still a long way from complete understanding of the disorder.
Key Terms
agoraphobia anxiety disorder characterized by intense fear, anxiety, and avoidance of situations in which it might be difficult to escape if one experiences symptoms of a panic attack
antisocial personality disorder characterized by a lack of regard for others’ rights, impulsivity, deceitfulness, irresponsibility, and lack of remorse over misdeeds
anxiety disorder characterized by excessive and persistent fear and anxiety, and by related disturbances in behavior
attention deficit/hyperactivity disorder childhood disorder characterized by inattentiveness and/or hyperactive, impulsive behavior
atypical describes behaviors or feelings that deviate from the norm
autism spectrum disorder childhood disorder characterized by deficits in social interaction and communication, and repetitive patterns of behavior or interests
bipolar and related disorders group of mood disorders in which mania is the defining feature
bipolar disorder mood disorder characterized by mood states that vacillate between depression and mania
body dysmorphic disorder involves excessive preoccupation with an imagined defect in physical appearance
borderline personality disorder instability in interpersonal relationships, self-image, and mood, as well as impulsivity; key features include intolerance of being alone and fear of abandonment, unstable relationships, unpredictable behavior and moods, and intense and inappropriate anger
catatonic behavior decreased reactivity to the environment; includes posturing and catatonic stupor
comorbidity co-occurrence of two disorders in the same individual
delusion belief that is contrary to reality and is firmly held, despite contradictory evidence
depersonalization/derealization disorder dissociative disorder in which people feel detached from the self (depersonalization), and the world feels artificial and unreal (derealization)
depressive disorder one of a group of mood disorders in which depression is the defining feature
diagnosis determination of which disorder a set of symptoms represents
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) authoritative index of mental disorders and the criteria for their diagnosis; published by the American Psychiatric Association (APA)
diathesis-stress model suggests that people with a predisposition for a disorder (a diathesis) are more likely to develop the disorder when faced with stress; model of psychopathology
disorganized thinking disjointed and incoherent thought processes, usually detected by what a person says
disorganized/abnormal motor behavior highly unusual behaviors and movements (such as child-like behaviors), repeated and purposeless movements, and displaying odd facial expressions and gestures
dissociative amnesia dissociative disorder characterized by an inability to recall important personal information, usually following an extremely stressful or traumatic experience
dissociative disorders group of DSM-5 disorders in which the primary feature is that a person becomes dissociated, or split off, from his or her core sense of self, resulting in disturbances in identity and memory
dissociative fugue symptom of dissociative amnesia in which a person suddenly wanders away from one’s home and experiences confusion about his or her identity
dissociative identity disorder dissociative disorder (formerly known as multiple personality disorder) in which a person exhibits two or more distinct, well-defined personalities or identities and experiences memory gaps for the time during which another identity emerged
dopamine hypothesis theory of schizophrenia that proposes that an overabundance of dopamine or dopamine receptors is responsible for the onset and maintenance of schizophrenia
etiology cause or causes of a psychological disorder
flashback psychological state lasting from a few seconds to several days, during which one relives a traumatic event and behaves as though the event were occurring at that moment
flight of ideas symptom of mania that involves an abruptly switching in conversation from one topic to another
generalized anxiety disorder characterized by a continuous state of excessive, uncontrollable, and pointless worry and apprehension
grandiose delusion characterized by beliefs that one holds special power, unique knowledge, or is extremely important
hallucination perceptual experience that occurs in the absence of external stimulation, such as the auditory hallucinations (hearing voices) common to schizophrenia
harmful dysfunction model of psychological disorders resulting from the inability of an internal mechanism to perform its natural function
hoarding disorder characterized by persistent difficulty in parting with possessions, regardless of their actual value or usefulness
hopelessness theory cognitive theory of depression proposing that a style of thinking that perceives negative life events as having stable and global causes leads to a sense of hopelessness and then to depression
International Classification of Diseases (ICD) authoritative index of mental and physical diseases, including infectious diseases, and the criteria for their diagnosis; published by the World Health Organization (WHO)
locus coeruleus area of the brainstem that contains norepinephrine, a neurotransmitter that triggers the body’s fight-or-flight response; has been implicated in panic disorder
major depressive disorder commonly referred to as “depression” or “major depression,” characterized by sadness or loss of pleasure in usual activities, as well other symptoms
mania state of extreme elation and agitation
manic episode period in which an individual experiences mania, characterized by extremely cheerful and euphoric mood, excessive talkativeness, irritability, increased activity levels, and other symptoms
mood disorder one of a group of disorders characterized by severe disturbances in mood and emotions; the categories of mood disorders listed in the DSM-5 are bipolar and related disorders and depressive disorders
negative symptom characterized by decreases and absences in certain normal behaviors, emotions, or drives, such as an expressionless face, lack of motivation to engage in activities, reduced speech, lack of social engagement, and inability to experience pleasure
neurodevelopmental disorder one of the disorders that are first diagnosed in childhood and involve developmental problems in academic, intellectual, social functioning
obsessive-compulsive and related disorders group of overlapping disorders listed in the DSM-5 that involves intrusive, unpleasant thoughts and/or repetitive behaviors
obsessive-compulsive disorder characterized by the tendency to experience intrusive and unwanted thoughts and urges (obsession) and/or the need to engage in repetitive behaviors or mental acts (compulsions) in response to the unwanted thoughts and urges
orbitofrontal cortex area of the frontal lobe involved in learning and decision-making
panic attack period of extreme fear or discomfort that develops abruptly; symptoms of panic attacks are both physiological and psychological
panic disorder anxiety disorder characterized by unexpected panic attacks, along with at least one month of worry about panic attacks or self-defeating behavior related to the attacks
paranoid delusion characterized by beliefs that others are out to harm them
peripartum onset subtype of depression that applies to women who experience an episode of major depression either during pregnancy or in the four weeks following childbirth
persistent depressive disorder depressive disorder characterized by a chronically sad and melancholy mood
personality disorder group of DSM-5 disorders characterized by an inflexible and pervasive personality style that differs markedly from the expectations of one’s culture and causes distress and impairment; people with these disorders have a personality style that frequently brings them into conflict with others and disrupts their ability to develop and maintain social relationships
posttraumatic stress disorder (PTSD) experiencing a profoundly traumatic event leads to a constellation of symptoms that include intrusive and distressing memories of the event, avoidance of stimuli connected to the event, negative emotional states, feelings of detachment from others, irritability, proneness toward outbursts, hypervigilance, and a tendency to startle easily; these symptoms must occur for at least one month
prodromal symptom in schizophrenia, one of the early minor symptoms of psychosis
psychological disorder condition characterized by abnormal thoughts, feelings, and behaviors
psychopathology study of psychological disorders, including their symptoms, causes, and treatment; manifestation of a psychological disorder
rumination in depression, tendency to repetitively and passively dwell on one’s depressed symptoms,
their meanings, and their consequences
safety behavior mental and behavior acts designed to reduce anxiety in social situations by reducing the chance of negative social outcomes; common in social anxiety disorder
schizophrenia severe disorder characterized by major disturbances in thought, perception, emotion, and behavior with symptoms that include hallucinations, delusions, disorganized thinking and behavior, and negative symptoms
seasonal pattern subtype of depression in which a person experiences the symptoms of major depressive disorder only during a particular time of year
social anxiety disorder characterized by extreme and persistent fear or anxiety and avoidance of social situations in which one could potentially be evaluated negatively by others
somatic delusion belief that something highly unusual is happening to one’s body or internal organs
specific phobia anxiety disorder characterized by excessive, distressing, and persistent fear or anxiety about a specific object or situation
suicidal ideation thoughts of death by suicide, thinking about or planning suicide, or making a suicide attempt
suicide death caused by intentional, self-directed injurious behavior supernatural describes a force beyond scientific understanding ventricle one of the fluid-filled cavities within the brain
Summary
What Are Psychological Disorders?
Psychological disorders are conditions characterized by abnormal thoughts, feelings, and behaviors. Although challenging, it is essential for psychologists and mental health professionals to agree on what kinds of inner experiences and behaviors constitute the presence of a psychological disorder. Inner experiences and behaviors that are atypical or violate social norms could signify the presence of a disorder; however, each of these criteria alone is inadequate. Harmful dysfunction describes the view that psychological disorders result from the inability of an internal mechanism to perform its natural function. Many of the features of harmful dysfunction conceptualization have been incorporated in the APA’s formal definition of psychological disorders. According to this definition, the presence of a psychological disorder is signaled by significant disturbances in thoughts, feelings, and behaviors; these disturbances must reflect some kind of dysfunction (biological, psychological, or developmental), must cause significant impairment in one’s life, and must not reflect culturally expected reactions to certain life events.
Diagnosing and Classifying Psychological Disorders
The diagnosis and classification of psychological disorders is essential in studying and treating psychopathology. The classification system used by most U.S. professionals is the DSM-5. The first edition of the DSM was published in 1952, and has undergone numerous revisions. The 5th and most recent edition, the DSM-5, was published in 2013. The diagnostic manual includes a total of 237 specific diagnosable disorders, each described in detail, including its symptoms, prevalence, risk factors, and comorbidity. Over time, the number of diagnosable conditions listed in the DSM has grown steadily, prompting criticism from some. Nevertheless, the diagnostic criteria in the DSM are more explicit than that of any other system, which makes the DSM system highly desirable for both clinical diagnosis and research.
Perspectives on Psychological Disorders
Psychopathology is very complex, involving a plethora of etiological theories and perspectives. For centuries, psychological disorders were viewed primarily from a supernatural perspective and thought to arise from divine forces or possession from spirits. Some cultures continue to hold this supernatural belief. Today, many who study psychopathology view mental illness from a biological perspective, whereby psychological disorders are thought to result largely from faulty biological processes. Indeed, scientific advances over the last several decades have provided a better understanding of the genetic, neurological, hormonal, and biochemical bases of psychopathology. The psychological perspective, in contrast, emphasizes the importance of psychological factors (e.g., stress and thoughts) and environmental factors in the development of psychological disorders. A contemporary, promising approach is to view disorders as originating from an integration of biological and psychosocial factors. The diathesis-stress model suggests that people with an underlying diathesis, or vulnerability, for a psychological disorder are more likely than those without the diathesis to develop the disorder when faced with stressful events.
Anxiety Disorders
Anxiety disorders are a group of disorders in which a person experiences excessive, persistent, and distressing fear and anxiety that interferes with normal functioning. Anxiety disorders include specific phobia: a specific unrealistic fear; social anxiety disorder: extreme fear and avoidance of social situations; panic disorder: suddenly overwhelmed by panic even though there is no apparent reason to be frightened; agoraphobia: an intense fear and avoidance of situations in which it might be difficult to escape; and generalized anxiety disorder: a relatively continuous state of tension, apprehension, and dread.
Obsessive-Compulsive and Related Disorders
Obsessive-compulsive and related disorders are a group of DSM-5 disorders that overlap somewhat in that they each involve intrusive thoughts and/or repetitive behaviors. Perhaps the most recognized of these disorders is obsessive-compulsive disorder, in which a person is obsessed with unwanted, unpleasant thoughts and/or compulsively engages in repetitive behaviors or mental acts, perhaps as a way of coping with the obsessions. Body dysmorphic disorder is characterized by the individual becoming excessively preoccupied with one or more perceived flaws in his physical appearance that are either nonexistent or unnoticeable to others. Preoccupation with the perceived physical defects causes the person to experience significant anxiety regarding how he appears to others. Hoarding disorder is characterized by persistent difficulty in discarding or parting with objects, regardless of their actual value, often resulting in the accumulation of items that clutter and congest her living area.
Posttraumatic Stress Disorder
Posttraumatic stress disorder (PTSD) was described through much of the 20th century and was referred to as shell shock and combat neurosis in the belief that its symptoms were thought to emerge from the stress of active combat. Today, PTSD is defined as a disorder in which the experience of a traumatic or profoundly stressful event, such as combat, sexual assault, or natural disaster, produces a constellation of symptoms that must last for one month or more. These symptoms include intrusive and distressing memories of the event, flashbacks, avoidance of stimuli or situations that are connected to the event, persistently negative emotional states, feeling detached from others, irritability, proneness toward outbursts, and a tendency to be easily startled. Not everyone who experiences a traumatic event will develop PTSD; a variety of risk factors associated with its development have been identified.
Mood Disorders
Mood disorders are those in which the person experiences severe disturbances in mood and emotion. They include depressive disorders and bipolar and related disorders. Depressive disorders include major depressive disorder, which is characterized by episodes of profound sadness and loss of interest or pleasure in usual activities and other associated features, and persistent depressive disorder, which marked by a chronic state of sadness. Bipolar disorder is characterized by mood states that vacillate between sadness and euphoria; a diagnosis of bipolar disorder requires experiencing at least one manic episode, which is defined as a period of extreme euphoria, irritability, and increased activity. Mood
disorders appear to have a genetic component, with genetic factors playing a more prominent role in bipolar disorder than in depression. Both biological and psychological factors are important in the development of depression. People who suffer from mental health problems, especially mood disorders, are at heightened risk for suicide.
Schizophrenia
Schizophrenia is a severe disorder characterized by a complete breakdown in one’s ability to function in life; it often requires hospitalization. People with schizophrenia experience hallucinations and delusions, and they have extreme difficulty regulating their emotions and behavior. Thinking is incoherent and disorganized, behavior is extremely bizarre, emotions are flat, and motivation to engage in most basic life activities is lacking. Considerable evidence shows that genetic factors play a central role in schizophrenia; however, adoption studies have highlighted the additional importance of environmental factors. Neurotransmitter and brain abnormalities, which may be linked to environmental factors such as obstetric complications or exposure to influenza during the gestational period, have also been implicated. A promising new area of schizophrenia research involves identifying individuals who show prodromal symptoms and following them over time to determine which factors best predict the development of schizophrenia. Future research may enable us to pinpoint those especially at risk for developing schizophrenia and who may benefit from early intervention.
Dissociative Disorders
The main characteristic of dissociative disorders is that people become dissociated from their sense of self, resulting in memory and identity disturbances. Dissociative disorders listed in the DSM-5 include dissociative amnesia, depersonalization/derealization disorder, and dissociative identity disorder. A person with dissociative amnesia is unable to recall important personal information, often after a stressful or traumatic experience.
Depersonalization/derealization disorder is characterized by recurring episodes of depersonalization (i.e., detachment from or unfamiliarity with the self) and/or derealization (i.e., detachment from or unfamiliarity with the world). A person with dissociative identity disorder exhibits two or more well- defined and distinct personalities or identities, as well as memory gaps for the time during which another identity was present.
Dissociative identity disorder has generated controversy, mainly because some believe its symptoms can be faked by patients if presenting its symptoms somehow benefits the patient in avoiding negative consequences or taking responsibility for one’s actions. The diagnostic rates of this disorder have increased dramatically following its portrayal in popular culture. However, many people legitimately suffer over the course of a lifetime with this disorder.
Personality Disorders
Individuals with personality disorders exhibit a personality style that is inflexible, causes distress and impairment, and creates problems for themselves and others. The DSM-5 recognizes 10 personality disorders, organized into three clusters. The disorders in Cluster A include those characterized by a personality style that is odd and eccentric. Cluster B includes personality disorders characterized chiefly by a personality style that is impulsive, dramatic, highly emotional, and erratic, and those in Cluster C are characterized by a nervous and fearful personality style. Two Cluster B personality disorders, borderline personality disorder and antisocial personality disorder, are especially problematic. People with borderline personality disorder show marked instability in mood, behavior, and self-image, as well as impulsivity. They cannot stand to be alone, are unpredictable, have a history of stormy relationships, and frequently display intense and inappropriate anger. Genetic factors and adverse childhood experiences (e.g., sexual abuse) appear to be important in its development. People with antisocial personality display a lack of regard for the rights of others; they are impulsive, deceitful, irresponsible, and unburdened by any sense of guilt. Genetic factors and socialization both appear to be important in the origin of antisocial personality disorder. Research has also shown that those with this disorder do not experience emotions the way most other people do.
Disorders in Childhood
Neurodevelopmental disorders are a group of disorders that are typically diagnosed during childhood and are characterized by developmental deficits in personal, social, academic, and intellectual realms; these disorders include attention deficit/hyperactivity disorder (ADHD) and autism spectrum disorder. ADHD is characterized by a pervasive pattern of inattention and/or hyperactive and impulsive behavior that interferes with normal functioning. Genetic and neurobiological factors contribute to the development of ADHD, which can persist well into adulthood and is often associated with poor long-term outcomes. The major features of autism spectrum disorder include deficits in social interaction and communication and repetitive movements or interests. As with ADHD, genetic factors appear to play a prominent role in the development of autism spectrum disorder; exposure to environmental pollutants such as mercury have also been linked to the development of this disorder. Although it is believed by some that autism is triggered by the MMR vaccination, evidence does not support this claim.
Review Questions
Which of the following is nota primary characteristic of ADHD?
- short attention span
- difficulty concentrating and distractibility
- restricted and fixated interest
- excessive fidgeting and squirming
One of the primary characteristics of autism spectrum disorder is ________.
- bed-wetting
- difficulty relating to others
- short attention span
- intense and inappropriate interest in others
Critical Thinking Questions
- Compare the factors that are important in the development of ADHD with those that are important in the development of autism spectrum disorder.
Personal Application Questions
- Discuss the characteristics of autism spectrum disorder with a few of your friends or members of your family (choose friends or family members who know little about the disorder) and ask them if they think the cause is due to bad parenting or vaccinations. If they indicate that they believe either to be true, why do you think this might be the case? What would be your response?
